
A Pound of Prevention? Women, Risk, and Alzheimer’s
American founding father Benjamin Franklin once said, “an ounce of prevention is worth a pound of cure.” This phrase is still popular in American culture today - and I imagine many other languages have similar expressions. But what happens when organizations encourage prevention strategies for diseases like Alzheimer’s that aren’t currently or completely preventable? And why are these prevention strategies so much more prominent in websites for women?
Women, Prevention, Risk, and Alzheimer’s
It is generally acknowledged in Alzheimer’s research and treatment that a larger number of women than men suffer from the disease, or that there is a higher prevalence rate in women. This rate is generally reported as approximately two thirds of patients (Moschetti et al. 2012, Mielke et al. 2014). However, there is much debate on what proportion of women have Alzheimer’s once differences in population are controlled - also known as the incidence rate.
Incidence rate more accurately communicates your average individual’s risk for the disease. Much of the research has shown that this higher prevalence rate is due to women living longer - meaning that ultimately, the incidence rate is the same (Moschetti et al. 2012, Fischer et al. 2018, Edland et al. 2002, Mielke et al. 2014.). However, some research has also found evidence to the contrary (Gao et al. 1998, Edland et al. 2002). Moreover, if there is a disparity in incidence, the causes behind this are elusive. Overall there is much about Alzheimer’s disease that needs further research.
There are a number of organizations devoted to research, informing patients and families, and raising awareness about Alzheimer’s. A subset of these websites and organizations are specifically focused on women. The focus here is on six websites dealing with women and Alzheimer’s disease. Samples were also taken from five gender non-specific Alzheimer’s and aging websites as a point of comparison. These platforms were approached using multimodal critical discourse analysis, that is, both written and visual elements were included in data collection. Important to multimodal analysis is analysis of how visual, textual, and other elements interact and are framed in relation to each other. While each mode operates in a specific way, when presented together they do not operate independent of each other.
Discourses about risk and risk management (prevention) were found to be more prominent and intense on websites aimed at women.
Moreover, color, font choices, structure of the website, and placement of images and text can all influence how we interpret information. Kress (2010) describes how, “each mode does a specific thing: image shows what takes too long to read, and writing names what would be difficult to show. Color is used to highlight specific aspects of the overall message” (p. 1). Whether information is meant to shock us or comfort us is communicated by far more than just the words themselves. Therefore multimodal analysis was employed in order to holistically interpret these websites.
The Two Thirds Statistic
Discourses about risk and risk management (prevention) were found to be more prominent and intense on websites aimed at women. Often these websites overemphasized the prevalence of Alzheimer’s in women - ⅔ of patients - while downplaying or outright ignoring the potential importance of incidence. By ignoring incidence, these websites heighten a discourse of risk and fear in a way that is not present in gender-neutral websites. Take for example the below image from the Women’s Alzheimer’s Movement (WAM) website:
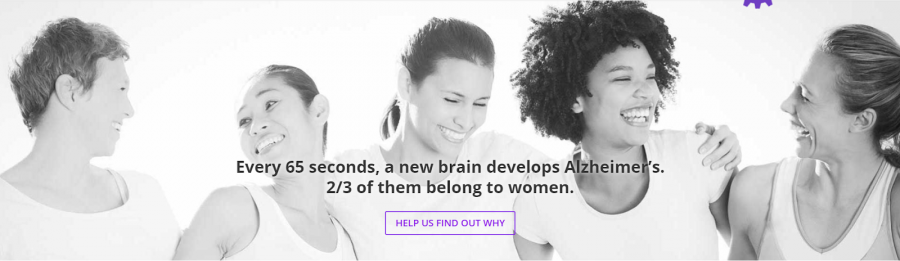
Notably, below the statement that ⅔ of Alzheimer’s sufferers are women, is a button (leading to a donation page) that states “help us find out why.” “Help us find out why” implies that there is little, if any, research explaining this statistic. Further, on WAM’s “about Alzheimer’s” page, it is stated again that “⅔ of those diagnosed are women - and no one knows why.” By ignoring not just the incidence qualifier but the existing research altogether, WAM constructs a very particular and perhaps the most extreme example of this discourse. In particular the use of the phrase “no one knows why” communicates a tone of fear via emphasis on the unknown and by extension the uncontrollable. This discourse relies on a compounding of uncertainty - that not only do women have some sort of inherent risk, but that there is no known method of mitigating that risk.
At first glance the background image seems lighthearted or meant to communicate a sense of camaraderie. However it also focuses on young women, who are usually not associated with Alzheimer’s, and women of different races. This communicates that the risk addressed in the text can affect anyone. Therefore the element of an uncontrollable risk is reinforced: because we don’t know why so many women are affected, no woman is safe.
Women and Alzheimer’s, a women-focused sub-project of the Cure Alzheimer’s Fund, takes a more subtle approach, but still communicates an alarming message:
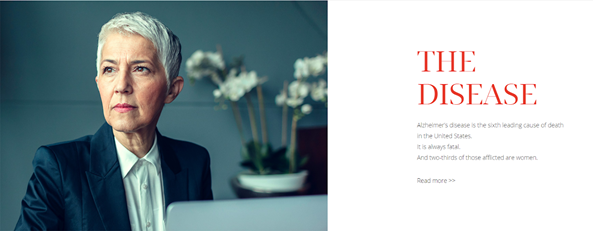
As an organization focused on funding research, Women and Alzheimer’s white background with blue and red accents mimics the color palette of a hospital or laboratory. The overall tone of both the parent and sub-site is one that is clinical and rather restrained. In this example, the large font, brightly colored writing belongs to “THE DISEASE” instead of a number or statistic. Here the two thirds statistic is paired with a statistic about death, and the statement that Alzheimer’s is always fatal. Therefore a discourse of risk is presented and reinforced by explicitly stating the outcome of that risk: death.
Additionally, the photo to the left is significant. In a pose seen somewhat frequently across both gender specific and non-specific platforms, a woman stares contemplatively into a distance we cannot see. We can only assume she is reflecting on her increased risk for Alzheimer’s, or perhaps even a recent diagnosis. The colors of the photo are muted blues and grays with bright lighting on her face. She is somber and contemplative. When paired with the text, the photo uses facial expression and color in order to communicate to the viewer a specific emotional response – a quiet determination in the face of fear.
Brain Food
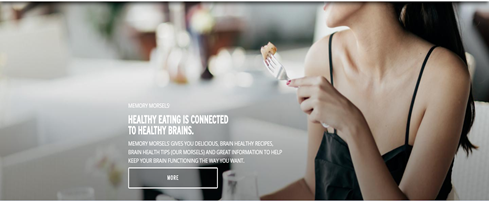
As counterbalance to this discourse of risk, many of the websites examined offer a discourse of risk management, mainly via prevention practices. Again, this discourse is heightened in gender-specific spaces. Take for example the Alzheimer’s Association’s (a gender non-specific organization) prevention page. They emphasize that “there are no clear-cut answers yet” and state “While research is not yet conclusive, certain lifestyle choices, such as physical activity and diet, may help support brain health and prevent Alzheimer's…” (Prevention, n.d.). Meanwhile, the front page of the Women’s Brain Health Initiative (WBHI) advertises their blog series called “Memory Morsels” which promises recipes and tips to “help keep your brain functioning the way you want.”
Placement within the website is significant. In the example comparison, WBHI places diet based prevention on the front page, whereas Alzheimer’s Associations’ prevention page is several clicks deep into the website. Further Alzheimer’s Association categorizes prevention under “Research and Progress” versus WBHI’s tone of relative certainty.
A discourse of prevention is one of actively fighting disease before one is even sick.
On another women’s website, the Women’s Alzheimer’s Movement, the “tips & tools” link is at the top of the front page. While it might be reasonable to assume these “tips and tools” are resources for families, or contain information on early symptoms, it in fact links directly to their “prevention” page.
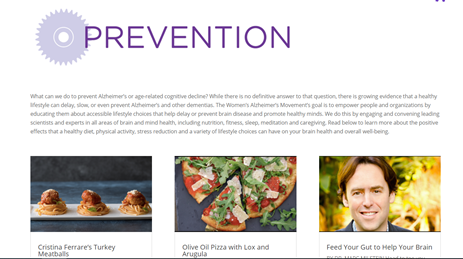
The prevention page from the Women’s Alzheimer’s Movement includes in small print that “there is no definitive answer” to Alzheimer’s prevention. However this statement is dwarfed by a) the word “Prevention” in large purple print and b) several large, brightly colored photographs. Two of these are images of food (representing recipes) and the third is a guest blog post on how to “feed your gut to help your brain.”
Of the 43 posts on the prevention page, 22 have to do with diet and/or exercise. The rest are scattered over meditation, staying socially engaged, and even an article on vitamins and supplements. Given larger cultural discourses that encourage women to stay slim through careful dieting and exercise, this emphasis is both logical and concerning. While sleep, stress, social engagement, and menopause treatment are significantly present in prevention discourses, there is an overwhelming emphasis on diet and exercise, particularly diet.
Prevention as Moral Obligation
A discourse of prevention is one of actively fighting disease before one is even sick. While of course no one is arguing against a healthy diet, this discourse becomes problematic when illness is seen as a failure of prevention. Prevention discourses construct health as social obligation, with a strong moral component. In the tradition of Foucauldian bio-power, Greco (1993) describes how sickness then becomes a failure of one’s “duty to be well.”
Galvin (2002) in their work on chronic illness describes how health has become “...no longer the absence of something bad, it is a positive entity all of its own, a state to be actively pursued” (p. 116). It is not enough to be merely not sick, but health, especially health intended as lifelong prevention, is a state in its own right. Maintaining this state is seen as a social and moral obligation.
When considering Alzheimer’s, a disease in which the underlying mechanisms are still not well understood, one might imagine a lessening of a duty to be well, or a submission to the whims of genetics. However, there is instead an intensification and dispersal of risk. Because prevention is not certain, efforts must be doubled. When risk, as with Alzheimer’s, is seen as uncontrollable, the paradoxical response is constant vigilance:
“Health-consciousness is also danger-consciousness - an awareness of and sensitivity to increasingly ambient and omnipresent potential harms. The ‘imperative of health’ is a mandate to identify dangers in order to control them. Most contemporary dangers to health, unlike an approaching epidemic, are not immediately apparent. Disease or symptoms may not appear for years, even decades. Both the pervasiveness of dangers and their prolonged time-span require a medically informed, vigilant and sustained awareness - a monitoring of the life-world for toxins, an ear turned to medical and governmental health advisories and, increasingly, a lifelong regimen of medical supervision. Thus, to be health conscious today is come into an understanding that one’s health is in continuous jeopardy.” (Crawford 2006, p. 403)
This discourse of extensive prevention practices is underwritten by one of risk dispersion. The wide net of preventative measures is drawn from the diverse efforts to uncover the underlying causes of Alzheimer’s and dementia. Any condition or lifestyle factor that has been researched in connection to Alzheimer’s, regardless of how early or (un)verified that research is, is reframed as a risk. Dispersed risk is transformed into dispersed prevention practices. Any research regarding underlying causes is represented as discovery of a new risk, and in turn transformed into a handbook to prevention.
For example, a popular refrain on Alzheimer’s websites, but one particularly highlighted on women’s websites, is that brain damage from Alzheimer’s can begin almost 20 years before one ever shows symptoms. This feeds into both the risk discourse - you can be sick and not even know it - and the prevention discourses - you need to start way before those 20 years! Thus Alzheimer’s websites construct a world in which one is always in danger of letting one's brain health slip, of not being vigilant enough in a world full of brain-destroying perils.
On women’s Alzheimer’s websites, the emphasis on risk and prevention is seemingly well intentioned but ultimately amounts to fear mongering and sometimes outright misinformation.
Lawless’ (2017) work on brain health advice in the media shows that similar discourses operate not just on websites directed at awareness raising for specific diseases, but in the news media more generally. Preventative brain health practices, and therefore the reduction or avoidance of dementia in old age, is framed as a choice - stay active, eat right, exercise, or suffer the consequences. Lawless states that “...by formulating brain health and illness in older age as logical outcome of individual practices, audiences are arguably positioned as logically accountable for the consequences of their actions" (2017, p. 69).
Greco (1993) points out that this notion of choice is often paradoxical - no one intentionally chooses to get sick, and even those who engage in a number of prevention practices may still get sick. This is especially true of Alzheimer’s - we still have very little understanding of how the disease works. And yet women’s organizations in particular push prevention strategies that may do nothing, reinforcing the social and moral obligation to maintain one’s health. In the context of larger cultural discourses on anti-aging and staying “healthy”- read: thin – that overwhelmingly focus on women, it makes sense that prevention discourses are also heightened on women’s websites. Women’s Alzheimer’s websites draw on the semiotic resources of larger cultural discourses to make their information on prevention accessible. Unfortunately, they fall into the same traps in the process.
A pound of prevention for an ounce of cure
Greco (1993) states that “the pursuit of ‘healthiness’ before disease conveys connotations of alarm and urgency: to ‘prevent’ becomes already to ‘cure’ something” (p. 360). On women’s Alzheimer’s websites, the emphasis on risk and prevention is seemingly well intentioned but ultimately amounts to fear mongering and sometimes outright misinformation. With a disease as devastating as Alzheimer’s it is tempting to cling to any promise of prevention – however these websites make promises that the body of research simply can’t support yet. No one is arguing against a healthy lifestyle – but it is misleading to think that it is an armor against all disease. Ultimately, websites intended to help are selling a pound of prevention for an ounce of cure.
References
Crawford, R. (2006). Health as a meaningful social practice. Health, 10(4), 401–420.
Edland, S. D., Rocca, W. A., Petersen, R. C., Cha, R. H., & Kokmen, E. (2002). Dementia and Alzheimer disease incidence rates do not vary by sex in Rochester, Minn. Archives of Neurology, 59(10), 1589–1593.
Fisher, Daniel W. ; Bennett, David A. ; Dong, H. (2018). Sexual dimorphism in predisposition to Alzheimer’s disease. Neurobiology of Aging, 70, 21.
Galvin, Rose (2002). Disturbing notions of chronic illness and individual responsibility: towards a genealogy of morals. Health, 6(2), 107–137.
Gao, Sujuan, Hendrie, Hugh, Hall, Kathleen, Hui, S. (1998). The Relationships Between Age, Sex, and the Incidence of Dementia and Alzheimer Disease. Archive of General Psychiatry, 55, 809–815.
Greco, M. (1993). Psychosomatic Subjects and the ‘Duty to be Well’: Personal Agency within Medical Rationality. Economy and Society, 22(3), 357–372.
Lawless, M., & Augoustinos, M. (2017). Brain health advice in the news: managing notions of individual responsibility in media discourse on cognitive decline and dementia. Qualitative Research in Psychology, 14(1), 62–80.
Mielke, M., Vemuri, P., & Rocca, W. (2014). Clinical epidemiology of Alzheimer’s disease: Assessing sex and gender differences. Clinical Epidemiology, 6(1), 37-48.
Moschetti, K., Cummings, P. L., Sorvillo, F., & Kuo, T. (2012). Burden of Alzheimer’s disease-related mortality in the United States, 1999-2008. Journal of the American Geriatrics Society, 60(8), 1509–1514.
Prevention. (n.d.).
WBHI Think Tank. (n.d.).
The Women's Alzheimer's Movement. (n.d.).
Women and Alzheimer's. (n.d.).